Why rehab handouts like these are missing the mark
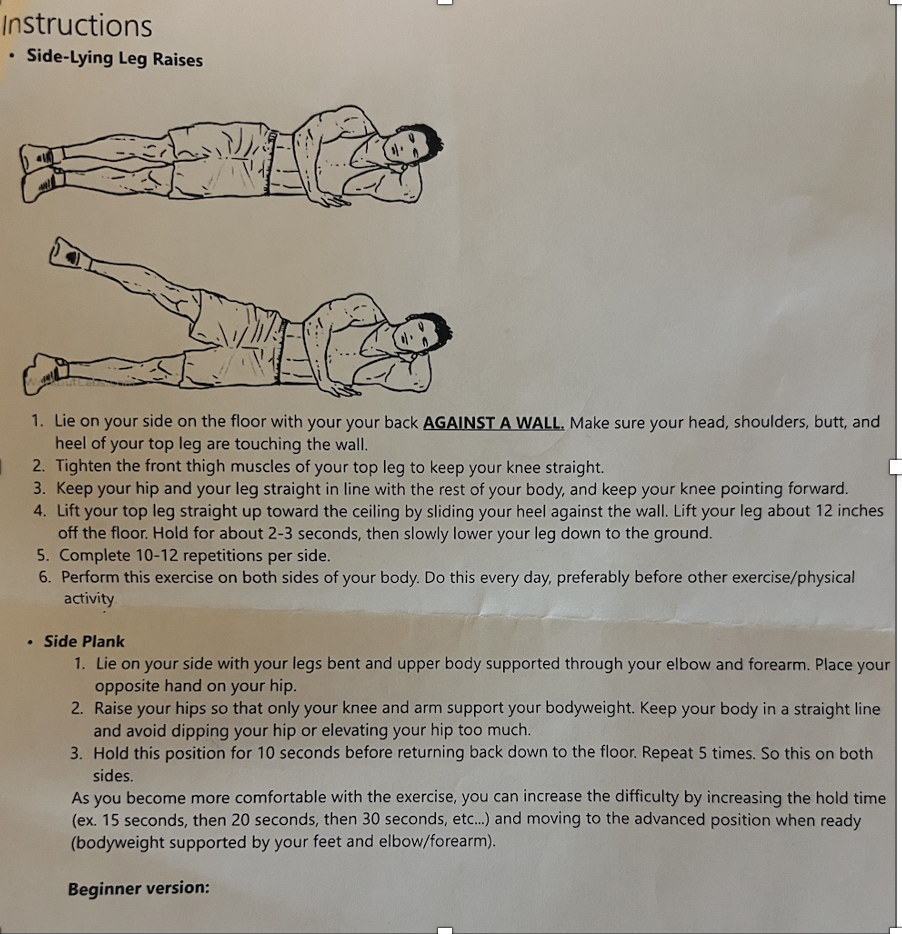
If you’ve ever left an ortho, physical therapy, or other sports medicine clinic with a black-and-white printout showing side-lying leg raises and side planks and wondered “am I doing this right?”, you are not alone. These exercises are often prescribed for low back, or hip pain, or knee pain. and on the surface, they seem reasonable. The problem isn’t that these exercises are wrong. The problem is that they are wildly insufficient as a standalone rehabilitation plan. This reality is where sports medicine fails in the United States. Much of this isn’t the fault of the practitioner, rather it is a result of a system driven by profit over patient outcomes.
Let’s talk about why black and white handouts are insufficient.
1. In this specific example, the prescribed exercise is not wrong, BUT did any
Yes, the gluteus medius abducts the hip but the glute med’s real job happens during:
Walking
Running
Cycling
Stair climbing
Load transfer through the pelvis
Lying on your side, sliding your heel up a wall, removes almost all the context that the glute med needs to function well: gravity management, ground reaction forces, pelvic control, and coordination with the trunk and foot.
You’re training a muscle in isolation that works as part of a system, the lumbo-pelvic hip complex. The patient needs to understand this and that this motion is the most basic component in an exercise progression. Doing side lying hip ABDuction is not going to cure hip pain.
2. These Exercises Don’t Screen for Why the Glute Med Isn’t Doing Its Job
Weakness is only one possible explanation for poor glute med contribution. Others include:
Pain inhibition
Poor motor control
Loss of hip internal rotation
Lumbar or pelvic asymmetry
Load management issues
Poor single-leg balance
Fear of movement
A handout assumes the diagnosis and the solution: Practitioners need to spend time to find the systemic underlying issues. A movement screen needs to be the foundational part of any good rehabilitative plan.
“Your glute med is weak. Do this.” Lacks a systemic plan or a rehab direction. The patient or athlete should always understand the why behind what you are doing and where we are going next in a rehab progression
3. Position ≠ Function
Side-lying leg raises and bent-knee side planks are:
Low-load
Low-variability
Highly constrained
They don’t challenge:
Pelvic drop control
Frontal-plane stability under fatigue
Hip-trunk dissociation
Reactive control
Speed or load progression
These exercises may be a good start after a surgical procedure or acute injury but, they don’t prepare someone to return to the very activities that usually triggered their symptoms. Rehab that doesn’t follow a load progression toward function isn’t rehab, it’s rehearsal.
4. No Guidance on Load, Tempo, or Progression
“10–12 reps.”
“Hold 10 seconds.”
“Do this every day.”
That’s not a program, that is merely a suggestion.
There’s no discussion of:
What “hard enough” should feel like
When to increase load
When to stop
What pain is acceptable
How this fits into walking, running, lifting, or sport
Without progression, tissue adaptation stalls. This is where insurance based orthopedic medicine falls short. Without load clarity, patients of poorly execute movements, under-dose and nothing changes or over-do it and can experience set-back. This is why all effective sports medicine should include specific guidance on load management at the very least. We highly recommend integrating guidance of a physical therapist, athletic trainer, or strength trainer as soon as possible in this process.
5. These Exercises Are Easy to Do Wrong—and No One Is Watching
Even experienced clinicians know how often these unintentionally turn into:
Hip flexor-dominant lifts
Lumbar side-bending instead of hip abduction
Pelvic rotation masquerading as “strength”
Neck and shoulder tension during side planks
A static image can’t cue breathing, alignment, or compensations.
And once bad reps are practiced daily, you’ve trained the wrong pattern very efficiently. Even a client who wants to be compliant likely needs one on one guidance to be successful.
6. They Ignore the Bigger Picture: The Entire Lateral Chain
The glute med doesn’t work alone. It cooperates with:
Quadratus lumborum
Adductors
Deep rotators
Core stabilizers
Foot and ankle mechanics
Rehab that only targets one muscle belly misses how force travels through the body. Pain and dysfunction are rarely single-muscle problems even if a single muscle is where the patient feels discomfort.
7. Education Without Individualization Isn’t Patient-Centered Care
Handouts like these are often given:
Without explaining why
Without relating them to the patient’s goals
Without acknowledging fear, frustration, or past failures
Patients deserve more than “do this forever.” And it is important that they understand that a handout like this is not training. Doing “rehab” exercises usually lacks enough overload to facilitate adaptation.
Your patient deserves:
Explanation and Understanding
Relevance
A plan that is dynamic and includes progressive loading
What Better Glute Med Rehab Actually Looks Like
Effective glute med rehabilitation:
Starts with assessment, not assumption
Progresses from bodyweight to functional loading
Incorporates single-leg tasks
Challenges balance and control
Integrates with walking, lifting, or sport
Adjusts based on adaptation, not just compliance
Side-lying leg raises and side planks can be a starting point—but they should never be the destination. At the Endurance Collective we strongly believe that any orthopedic rehab should include one on one movement and load guidance as soon as is possible in a rehab scenario. The bottom line is that these images aren’t harmful or wrong. They are just incomplete.
Rehab isn’t about collecting exercises, it’s about restoring capacity, confidence, and function. No injury gets better by practicing an over simplified routine without progression. If the goal is meaningful recovery, we owe patients more than a photocopy. Spend the time and you will see better outcomes.